


Trauma is a root cause behind many kinds of distress. For example, a significant share of cases of depression and anxiety can be traced back to trauma. Understanding trauma is essential for resolving persistent problems. Under medical supervision, a Certified Public Psychologist summarizes—in clear terms—what trauma (including developmental trauma) is, and what PTSD / Complex PTSD are. Please read on.
<Created: 2025.9.26 / Last Updated: 2025.9.26>
* If you wish to reprint or otherwise reuse content from this site, please credit the site name as the source or include a link back to this page.
 |
Author of this articleIchitaro Miki — Certified Public Psychologist Osaka University (BA); Osaka University Graduate School (MA) Over 20 years in psychological clinical practice. Specializes in trauma and attachment difficulties that underlie a wide range of problems and “ikizurasa” (chronic distress). Author of Developmental Trauma: The Real Cause of “Ikizurasa” and other books (approx. 40,000 copies in total), appearances on TV programs, clinical supervision for dramas, and numerous features in web media and magazines. |
|---|
Medical supervision for this articleDr. Yoshio Iijima (Psychosomatic Medicine, etc.) A psychosomatic physician who is also a licensed clinical psychologist, Kampo (traditional Japanese) physician, and general practitioner—well versed across disciplines. Specializes particularly in functional somatic symptoms and autonomic nervous system dysregulation. Click here for full profile |
<Editorial Policy>
・Written by a Certified Public Psychologist based on years of clinical experience and client narratives (especially from attachment- and trauma-informed perspectives). Provides explanations and key takeaways.
・References authoritative books and objective data to the best of our knowledge.
・Strives to incorporate the latest findings whenever possible.
・This article has been translated from the original Japanese using AI. Therefore, it may contain unnatural translations, particularly for specialized terms.
Contents
・What is trauma?
・(Reference) What is developmental trauma?
・(Reference) What is Developmental Trauma Disorder?
・Diagnostic criteria for trauma (PTSD / Complex PTSD)
・What experiences cause trauma?
・Main symptoms caused by trauma
・Healing and overcoming trauma
→ For related articles on trauma, please see below.
▶ “PTSD/Trauma, Stress, and Mental Care in Disasters (earthquakes, typhoons, accidents, etc.)”
▶ “Overcoming and Healing Trauma (Developmental Trauma), PTSD, and Complex PTSD”
What is trauma?
Stress disorders—common, everyday phenomena close to all of us
“Trauma” may sound dramatic and distant from one’s everyday life. In simple terms, however, trauma refers to stress disorders. Trauma exists on a spectrum, and mild forms are experienced by virtually everyone in daily life. When the severity reaches a moderate level, it is diagnosed as an “adjustment disorder (stress-related disorder),” and at higher severity as “acute stress disorder,” “PTSD,” “Complex PTSD,” or “dissociative disorders.” At some clinics, as many as 90% of visitors are said to present with stress-related disorders—this is how common they are.
→ Related articles
▶ “What is Adjustment Disorder? Understanding its Causes”
▶ “What are Dissociative Disorders and Dissociative Identity Disorder? Causes Explained”
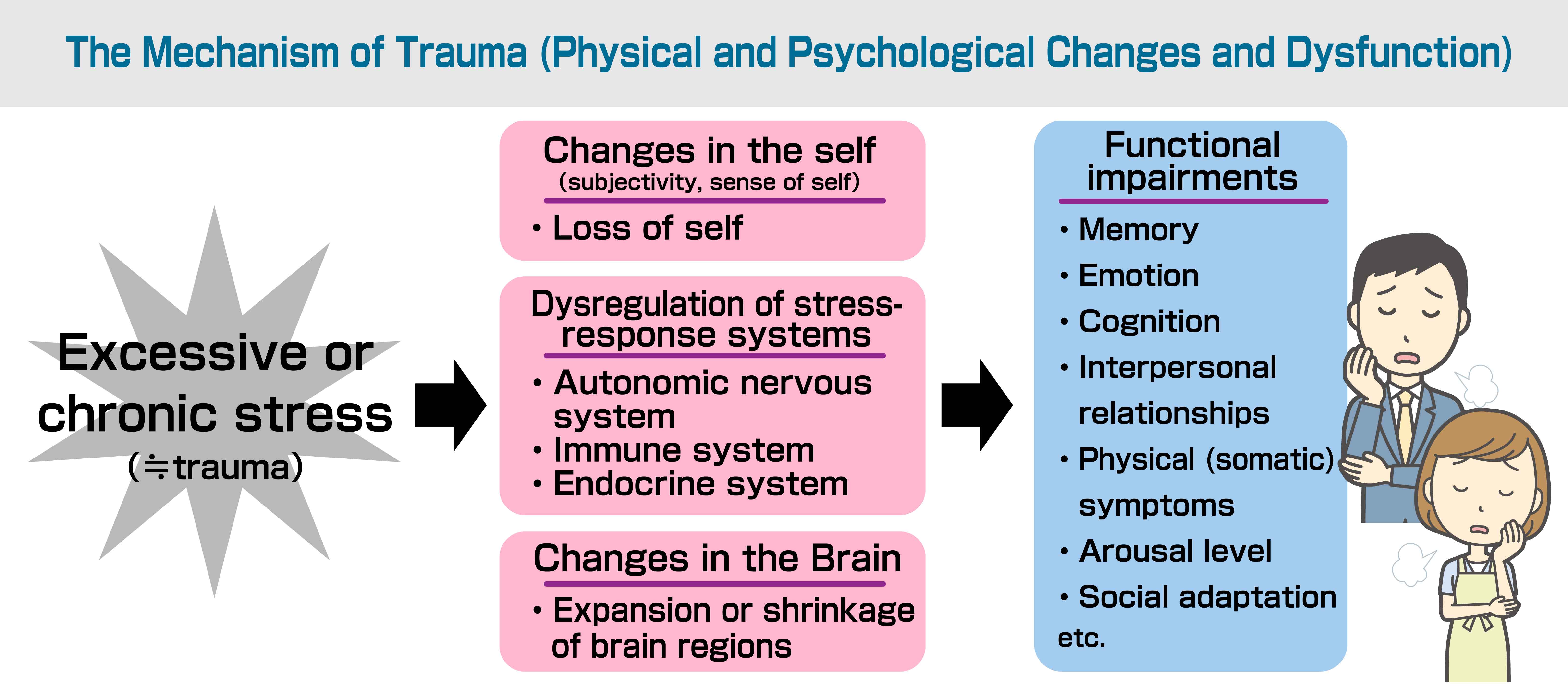
When an animal—including humans—encounters stress that exceeds the threshold of the stress-response system (meeting certain vulnerability conditions), dysregulation arises in the autonomic nervous system, immune system, and endocrine system. This affects domains such as emotion, arousal, cognition, body, and memory, resulting in diverse symptoms and a sense of “ikizurasa.”
As detailed below, trauma caused by a single, highly intense event such as a disaster or rape is called “single-incident trauma,” while trauma caused by prolonged, gradually accumulating stress is called “complex trauma.”
The human stress-response systems (autonomic, immune, endocrine) are not designed to cope with long-term stress. Therefore, even stress that appears mild on the surface can, when prolonged, cause dysfunction as severe as PTSD.
Another key feature of trauma—Harassment
Alongside stress disorders, another crucial perspective for understanding trauma is to recognize that “trauma is harassment.” In cases where people suffer long after the original events, the influence of harassment is almost always present.
Research on harassment traces back to anthropologist Gregory Bateson’s concept of the “double bind.” A double bind arises when contradictory messages are delivered simultaneously, disrupting a person’s free mental activity.
Bateson identified this as a cause of mental disorders. In everyday life, this includes situations in parent–child, partner, or supervisor–subordinate relationships where someone cloaks self-serving or deficit-driven behavior in plausible reasoning to make the other comply (false rules).
While the body and unconscious sense the other’s unfairness, the conscious mind is forced to accept it due to the seemingly reasonable logic—leading to compliance. Harassment, simply put, is the repetition of this pattern. Victims gradually lose trust in their own perceptions, become isolated from society, and end up controlled by the perpetrator.
Even with single-incident traumas such as accidents, disasters, wars, or rape, those who suffer for a long time almost invariably show the influence of harassment (e.g., social support deficits, secondary harassment). Harassment is a major psychological signature of trauma.
→ Related article
▶What Is Harassment (Moral Harassment)? — Causes and Characteristics
The core of trauma is the “loss of self”—Trauma robs us of being ourselves and creates chronic distress
At the heart of trauma’s impact lies the loss of self—the feeling that one’s self is taken away or has vanished. Trauma deprives us of being ourselves, eroding the fundamental sense that “I am mine.” This is especially pronounced in chronic trauma such as developmental trauma. There are several pathways to this loss: attachment insecurity (unstable relationships with caregivers), taking on family roles in dysfunctional families (e.g., young carers) at the expense of oneself, dysregulation of brain interoception, and interpersonal difficulties that prevent the self from being formed through relationships with others.
“A smartphone that isn’t logged in”
Many trauma survivors are active, resilient people who have survived adversity, so they would never imagine they “lack a self.” Physically they move, but it is as if they’re not logged in with their own ID. The body acts, but the self isn’t there; things don’t truly move by the self or become the self’s experience. As a result, experiences don’t accumulate; nothing feels like it becomes “mine.” This loss of self has been described as “like a display smartphone in an electronics store that isn’t logged in.” In severe trauma, this is strikingly evident. Many trauma-related symptoms can be understood as consequences of self-loss, where the mind and body cannot be properly governed.
Memory dysregulation—“Frozen memories” that stop time
Another lens on trauma is to view it as dysregulation of memory.
Ordinary memories are emotionally weighted by the amygdala, organized by the hippocampus, and stored. But extremely intense stress overactivates the amygdala, overwhelms hippocampal processing, and leaves memories fragmented and lingering out of conscious integration—often called “frozen memories.”
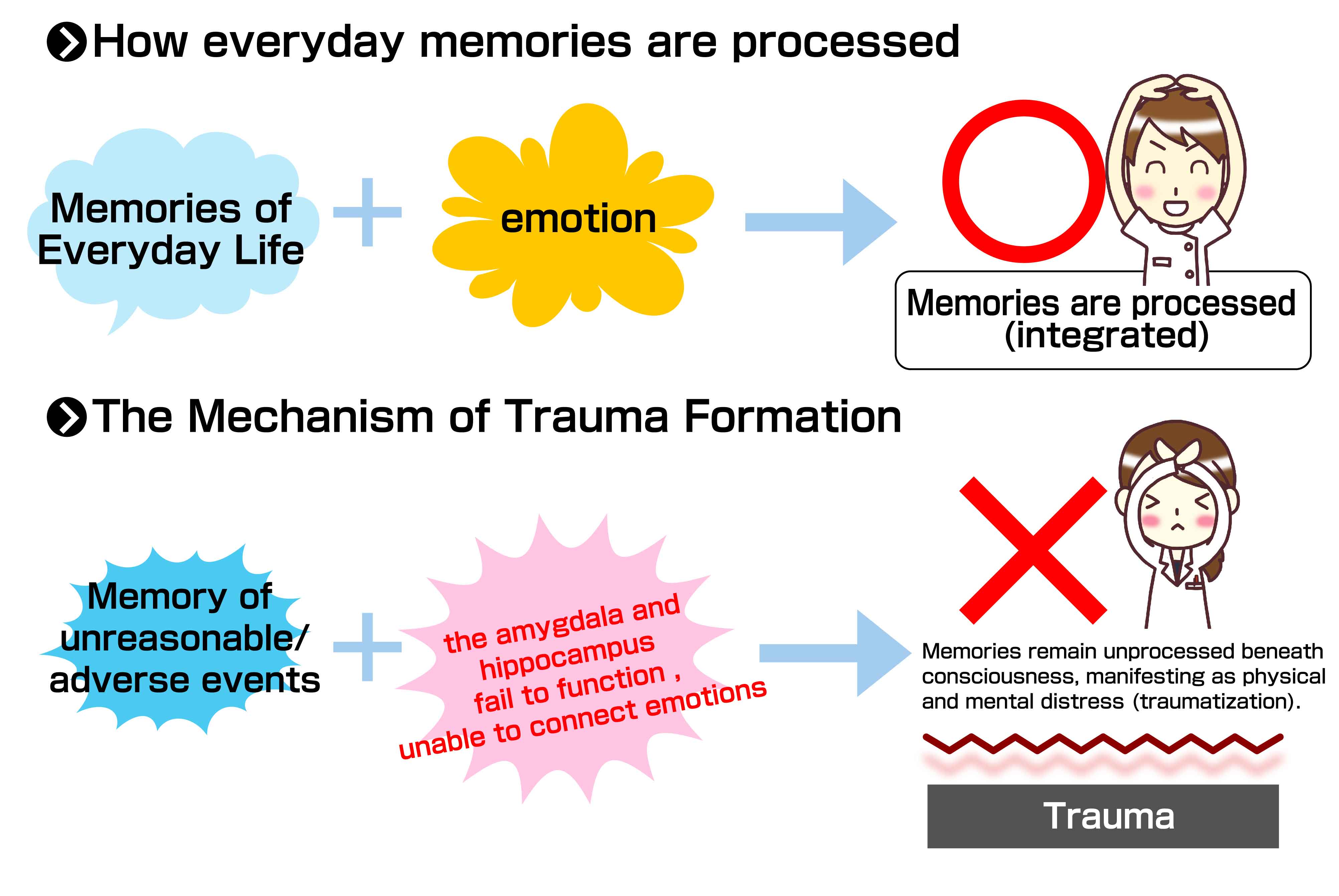
These “unprocessed memories” are thought to drive the phenomenon we call “trauma.” Like a time machine, physical time moves forward, yet the traumatic memory remains fresh; the person lives as if still in the past.
Two broad types of trauma (single-incident / complex)
Trauma can be categorized as:
1) Single-incident trauma: one-off, major stressors such as accidents, disasters, or rape
2) Chronic, repeated trauma (complex trauma): prolonged, repeated stressors such as inadequate caregiving, dysfunctional families, bullying, and harassment*
* Even seemingly minor stresses at home, school, or work can become traumatic when chronic.
Single-incident trauma is obviously serious; however, it is extremely common for people to carry complex trauma without recognizing it. It is no exaggeration to say that most people who seek help for persistent problems carry some form of trauma. Psychiatrist Judith Herman proposed Complex PTSD to describe trauma that cannot be fully explained by the traditional PTSD concept, and in 2018 it was officially adopted into the WHO’s International Classification of Diseases.
Reference: → Judith L. Herman, “Trauma and Recovery” (Misuzu Shobo, Japanese ed.)
(Reference) What is developmental trauma?
Developmental trauma refers to trauma incurred during the developmental years—primarily in childhood (though the clinically relevant window is handled flexibly). Concrete examples include inadequate caregiving, bullying, and the effects of dysfunctional families.
(Reference) What is Developmental Trauma Disorder?
Developmental Trauma Disorder is a proposed diagnosis intended to appropriately capture the wide range of symptoms that appear when a child experiences complex, repeated trauma. Arising from developmental-stage trauma, it can present as ADHD-like symptoms, conduct problems, dissociation, etc., and often culminates in Complex PTSD. It has not yet been formally adopted as a diagnostic criterion. While the terms sound similar, “Developmental Trauma Disorder” specifically proposes criteria for children exposed to inadequate caregiving and related adversities.
Diagnostic criteria for trauma (PTSD / Complex PTSD)
Below is a summary of diagnostic criteria for trauma.
・PTSD criteria
・Exposure—acute or repeated, and sometimes prolonged—to experiences involving extreme threat or fear, in which escape is difficult or impossible.
(Disasters, war, violence, torture, abuse, rape, etc.; not limited to these.)
When the three symptom clusters below persist for several weeks (under APA criteria, PTSD is diagnosed after symptoms persist > 1 month; < 1 month is “Acute Stress Disorder”).
1) Re-experiencing: reliving the traumatic event (flashbacks, nightmares, etc.)
The traumatic event is repeatedly relived. Severity varies widely. Unlike ordinary recall, re-experiencing is intrusive and vividly engages the senses. Rather than being remembered as past, it is felt as if happening now. Experiencing it as happening now is called a “flashback,” while during sleep it appears as “nightmares,” and in thought as “intrusive symptoms.” Children may reenact the trauma in play. *Flashbacks vary in degree and content.
2) Avoidance: avoiding reminders of the traumatic event
People try to avoid situations or individuals that evoke the trauma. Degrees vary—from explicit avoidance to vague reluctance or aversion. Some change jobs, schools, or residences.
3) Sense of current threat
A persistent sense that danger is still present nearby, and that one might be suddenly threatened. Even without conscious awareness, this may appear as chronic over-tension, bodily stiffness, fatigue, over-accommodation to avoid risk (overadaptation), hyperarousal, sleep problems, social/relationship fears, and more.
Reference: Under the APA’s DSM-5-TR (Igaku-Shoin, Japanese ed.), negative alterations in mood and cognition (e.g., persistent negative beliefs) are also included.
・Complex PTSD criteria
When the above three PTSD clusters (1–3) are present plus the following three, Complex PTSD is diagnosed. *Clinically, some flexibility is applied; the point is that, in addition to the PTSD clusters, the following three are characteristic of Complex PTSD—often summarized as “3 + 3.”
4) Disturbances in emotion regulation
Emotions become overly intense, explosive, or expressed in self-destructive behavior; conversely, emotions may be numbed or dissociated, with diminished access to positive feelings.
5) Persistent negative self-concept
Enduring feelings of worthlessness or insignificance; shame, guilt, defeat.
6) Disturbances in relationships
Difficulties forming relationships; avoiding or devaluing closeness and social engagement; trouble maintaining relationships; sudden surges of shame, fear, or anger that trigger “reset” urges, etc.
Reference: ICD-11
Want to know whether trauma may be affecting you? Try the simple self-check below.
(Reference) → “Trauma(Developmental Trauma, complex PTSD) Check for Self-Understanding”
What experiences cause trauma?
・Trauma arises when experiences exceed the threshold of the stress-response system (given certain vulnerability factors)
Traditionally, “traumatic experiences” referred to catastrophes such as train accidents or war, or to rape and abuse. The APA’s DSM-5-TR describes exposure to actual or threatened death, serious injury, or sexual violence (direct experience, witnessing, or learning of it). In reality, even ordinary events can become traumatic when, under certain environmental conditions, they exceed an individual’s stress-response threshold (i.e., vulnerability variables), especially over time.
Stress (event) + Individual sensitivity (resilience) + Environment (vulnerability variables) = Trauma
is a useful way to understand it.
・What counts as a traumatic experience?—Everyday stressors such as marital conflict or dysfunctional families are key causes
What used to be dismissed—like parents’ shouting matches—are now officially recognized as abuse under the label “witnessed domestic violence.” Some studies indicate that the combination of witnessing DV and verbal abuse causes the most severe damage—even more than physical abuse or neglect.
Beyond that, chronic, everyday stressors—dysfunctional families, bullying, harassment, and the absence of appropriate communication—are major causes of trauma. Stress research shows that prolonged stress without foreseeable relief leads to stress disorders; seemingly “small things,” when chronic, can indeed become traumatic.
(Reference) Trauma is not a single, specific event
In counseling, people sometimes ask, “What is my trauma?”—a common misconception. Trauma is not, by default, a single event. As noted above, it refers to the overall environment and experiences that produce a stress disorder. And difficulties are almost always multi-causal. Clinically, cases attributable to one discrete event alone are actually rare.
Main symptoms caused by trauma
・Chronic over-tension—unable to stay calm and be yourself
The most familiar symptom is chronic over-tension. Even in non-stressful situations, you tense up excessively. Willpower cannot control it; trying not to be tense often makes it worse. You end up constantly on edge, over-accommodating others, unable to relax. Internally, you’re exhausted. You may have trouble falling asleep. Trauma prevents you from being yourself.
→ Related article
▶ “Is Your Constant Tension a Result of Trauma?”
・Overadaptation
Overadaptation means “excessive people-pleasing” or “overfitting to others.” Trauma survivors habitually think several steps ahead, over-reading others’ feelings and thoughts. In groups, they over-manage logistics and take care of everyone.
・Fear of abandonment
Rooted in a lack of basic safety and trust—and low self-confidence—fear of abandonment fuses the survival of a relationship with one’s own existence. One’s self-worth becomes contingent on others’ evaluations and approval.
This drives excessive rumination, self-blame, and anxiety about one’s behavior; it also keeps people stuck in relationships that ought to end. Even when they “know” it’s okay to leave, anxiety binds them to the other.
→ Related article
▶ “Is Trauma the Hidden Cause of Your Relationship Problems?”
・Flashbacks
Traumatic events are repeatedly relived. You may ruminate, feel waves of shame, self-blame, or guilt, or have panic attacks. Recent memories can be distorted by flashbacks (e.g., “they laughed at me,” “they said something awful”). Overwhelming “shame flashbacks” or “self-blame flashbacks” are common—like sudden urges to cover your face or exclaim “ugh!” Self-harm impulses may also arise as (maladaptive) attempts to counter flashbacks.
・Diminished sense of safety and basic trust
Unprocessed past stress keeps danger ever-present. Even if your mind “knows” things are safe, your body and unconscious don’t. People may not recognize this underlying deficit; they may just see themselves as timid or blame “annoying others.” Lack of safety affects worldview and fosters negative cognitions.
・Social / interpersonal fears
People and society feel unsafe. The feared targets may resemble past perpetrators/situations, or fear may become generalized.
・Difficulty relating naturally; lack of felt connection
Trauma undermines relationship-building. Over-tension, overadaptation, abandonment fear, social fear, and self-loss interact to create pervasive interpersonal difficulties.
→ Related article
▶ “Is Trauma the Hidden Cause of Your Relationship Problems?”
・Sensory hypersensitivity or numbing
People may become hypersensitive to light or sound; wind or shower water can feel painful; certain smells become intolerable; touch becomes aversive; even proximity to others feels unbearable. Some cases labeled “HSP” may actually be trauma-related. Conversely, to avoid pain triggered by traumatic memories, sensations may be dulled, with a felt “membrane” separating oneself from the world; affect may be blunted. Interactions can feel delayed or effortful.
・Not recognizing or expressing emotions; aversion to emotions
Emotions can become difficult to access or express; affect and facial expression/behavior decouple. When voicing opinions, people reflexively think, “What’s normal? What do others feel?”—unconsciously over-reading others. Preferences become unclear. Past ridicule or suppression of genuine feelings (and harm-avoidant compulsions) can make it hard to feel or express warranted anger. Some develop aversion to being emotional.
What one intends to say can come out differently. It can feel like riding in a “broken robot”—unable to see and respond fluidly to the outside world.
・Dissociation, depersonalization, derealization
Dissociation is weakened integration of the self: depersonalization, derealization, and amnesia. “I don’t feel like myself,” “I feel like I’m watching myself from outside,” “as if there’s a thin film between me and the world,” “the world looks artificial.” Severe cases may lead to DID or conversion symptoms.
→ Related article
▶ “What are Dissociative Disorders and Dissociative Identity Disorder? Causes Explained”
・Hyperarousal
The brain and sympathetic nervous system are constantly revved up; relaxation and natural ease become elusive. Restlessness impedes steady work or study. Some even wish they could “take out the brain and wash it in cold water.” With chronically taut nerves, irritability and hyperactivity can appear. The issue is not “poor concentration” but too many simultaneous stimuli to focus on one. Symptoms may resemble ADHD. Tension also hinders sleep, causing insomnia or light sleep.
→ Related article
▶ “Causes and Diagnosis of Insomnia & Sleep Disorders—A Six-Lens Check”
・Negative cognitions/mood; twisted worldview
People may see themselves as worthless, blame themselves excessively, feel intense guilt/shame, resent others, and regard society as dangerous—often with depressive states.
A twisted worldview might include beliefs like “enduring unfairness is how you grow,” “you must never run away,” “I was abused because I’m a bad person,” “I wasn’t wanted in this world,” or “people who act unfairly are actually good and loving.” One may assume “they’re secretly angry” even when they seem pleased. Perpetrators’ justifications (“you’re a bad kid,” “it’s for your own good”) also reinforce distortion.
・A sense of “infinite” obligation
Healthy worlds run on finite cycles; traumatized worlds feel “infinite.” People feel infinitely bound by duty, guilt, or responsibility. They avoid separation at all costs, assume others’ problems as their own, and—fueled by abandonment fear—maintain relationships indefinitely. They may also overwork to the point of harming their health. Addictions and eating disorders rooted in trauma and deficiency are also “infinite” worlds without satiety.
・Blurred self–other boundaries
Trauma can blur the line between self and others. Due to attachment insecurity and violations of personal boundaries, people lose track of appropriate distance and responsibility. Overadaptation leads them to treat others’ feelings and roles as their own responsibility. Establishing boundaries feels “cold” or “bad.” Many do not notice this until a counselor points it out.
・Lack of confidence; stigma
People feel chronically insecure, fundamentally flawed, sinful, or wrong. Success or “positive thinking” doesn’t change this. They sense an indelible stigma or “taint.” When they attribute the cause of terrible experiences to themselves (“I was a bad child, so it happened”), they end up carrying a stigma.
・Impaired ability and performance—work or study suffers
Massive trauma-related memory constantly occupies working memory, diverting resources from the here-and-now—like a computer slowed by too many background processes. People struggle to grasp the big picture, get stuck on edge cases, fail to intuitively organize information, dislike numbers/calculation/tidying, lack confidence with simple tasks, and make frequent careless mistakes.
→ Related article
▶ “When Work Doesn’t Go Well: The Hidden Impact of Trauma”
・Idealism
Many trauma survivors become highly idealistic—aiming to transcend the “ugliness” they’ve endured. Rather than embracing pluralism, they gravitate toward a single, dominating ideal, and feel anger or frustration when reality diverges from it.
・Missing the “unspoken rules”; being swayed by others’ words
Trauma makes it hard to read the unspoken. People get caught by surface words. While they over-anticipate others’ feelings, they miss genuine nuance and subtext, both at work and in private life.
・Difficulty with self-disclosure; life “never starts”; fear of responsibility
People avoid genuine self-expression and shy away from responsibility at work due to fears of sudden attack or criticism. It can feel as if their own life never quite begins.
・Excessive “objectivity”
They feel compelled to reference some external absolute standard. Instead of responding from their own feelings/thoughts, they habitually ask, “What would others think?” Believing subjectivity is “bad” and objectivity “good,” they end up deferring to the loudest outside voices—though no absolute objectivity actually exists.
・Stolen time—pseudo-maturity, frozen time, and urgency
Trauma stalls the flow of time. People feel younger than peers, may even look younger, and feel “immature.” They may also seem precocious, having overadapted early to unfairness. True maturation requires phases of ego-satisfaction and rebellion; overadaptation blocks this, yielding a merely “pseudo-mature” shell. Because memory isn’t updated, their worldview and view of people remain stuck at the time of trauma (“shameful me, horrible others”). Trauma robs not only the self but also one’s sovereignty over time.
There is also a constant sense of being hurried—“I must do something to improve myself right now,” “I shouldn’t idle away.” One worries about the future rather than settling into the present; time never feels like one’s own.
・Memory loss
To protect against traumatic shock, memory may be repressed, leaving gaps. Like sealing a ship’s bulkheads after a breach to prevent sinking, the mind restricts access to overwhelming memories. If past memories feel unusually thin, consider repression.
・Lack of continuity—skills and experience don’t accumulate; everyday life feels empty
Trauma keeps crisis ever at hand, disrupting continuity across cognition (trust in “how things usually go”), relationships, roles/functions, and a coherent personal history. Without continuity, people live from moment to moment, feel their skills and experience never build, and find daily life joyless.
→ Related article
▶ “When Work Doesn’t Go Well: The Hidden Impact of Trauma”
・Panic symptoms from conflicts or flashbacks
Panic is common among those long subjected to interpersonal stress and harassment. Attempting to maintain conflicting beliefs or endurance strategies in the face of others’ whims and unfairness breeds inner conflict that can erupt as panic.
Strong flashbacks can also trigger panic—with hyperventilation and sudden sweating.
→ Related article
▶ “What Causes Panic Disorder? Endogenous Theories and “Conflict-Driven Panic””
・Reenacting one’s trauma
People may unconsciously recreate their trauma as victim or perpetrator. Those sexually abused may enter harmful sexual relationships or sex work; those neglected or controlled may repeat similar relationships—or become controlling themselves. This is not “attraction” due to personal fault. Rather, the brain/body “knows” that re-experiencing and properly processing memories could resolve them. Unfortunately, reenactments rarely occur in safe contexts, so trauma persists.
・Addictions / habitual dependencies
Trauma is known to fuel addictions. These are not about weakness but “immature self-treatment” attempts to relieve deficiency and distress—using alcohol, gambling, drugs, etc., to soothe fear, anxiety, loneliness, tension, or arousal triggered by trauma.
→ Related article
▶ “What is Addiction (e.g., Alcohol)? Types, Features, Mechanisms”
・Neurodevelopmental-like symptoms—“The fourth developmental disorder”
Unprocessed traumatic memory hogs cognitive resources, leaving only a fraction of working memory for daily tasks—producing ADHD-like symptoms (poor recall at work, frequent mistakes, inattention).
Overadaptation and chronic tension also impair social ease. With time “stopped,” self- and other-images remain immature.
With no spare capacity, developmental unevenness stands out, making symptoms closely resemble neurodevelopmental disorders—hence the notion of a “fourth developmental disorder.” Some diagnosed as neurodevelopmental may, in fact, reflect trauma-related presentations.
・Other presentations
Physical: sleep disorders, functional somatic symptoms, headaches, back pain, other bodily pain, autoimmune disease, diabetes, myocardial infarction, stroke, increased cancer risk, etc.
Mental: depressive states, anxiety disorders, emotion regulation problems, OCD, self-harm (e.g., cutting), suicidal ideation, personality disorders, eating disorders, bipolar disorder, conduct problems, dissociative disorders (incl. DID in severe cases), etc. As trauma literacy spreads, many conditions previously labeled differently are being reconsidered as potentially trauma-related.
(Reference) Trauma responses in children
These often differ from adult presentations:
・Overly adult-like speech/behavior (polite speech to conceal harm)
・Hyperactivity / aggression
・Sexualized behavior (heightened interest or repeated sexualized acts)
・Developmental delays (lagging age-appropriate milestones)・Behavioral problems (delinquency, bullying, etc.)
・Attachment disturbances (excessive clinging, avoidance, difficult reactions)…and more.
Healing and overcoming trauma
For approaches to healing and overcoming trauma, see the page below:
▶ “Overcoming and Healing Trauma (Developmental Trauma), PTSD, and Complex PTSD”
* If you wish to reprint or otherwise reuse content from this site, please credit the site name as the source or include a link back to this page.
(References / Sources)
Judith L. Herman, “Trauma and Recovery” (Misuzu Shobo, Japanese ed.)
Ichitaro Miki, Developmental Trauma: The Real Cause of “Ikizurasa” (Discover Keisho)
Hiroko Mizushima, “Understanding Psychological Trauma & PTSD” (Gijutsu-Hyoronsha)
Shigeki Mori, “Discovery of Trauma” (Kodansha)
Naoko Miyaji, “Trauma” (Iwanami Bunko)
Nozomu Asukai, “All About PTSD and Trauma” (Kodansha)
Kenichiro Okano, “New Traumatic Disorders” (Iwasaki Academic Press)
Quarterly Be! (Ask Human Care), Sept. 2015
Miyako Shirakawa, “Trauma Care of Little Red Riding Hood and the Wolf” (Ask Human Care)
Akemi Tomoda, “Attachment and Abuse,” in Neuroscience of Brain Development (Shin-yo-sha)
Bessel van der Kolk, “The Body Keeps the Score” (Kinokuniya, Japanese ed.)
Masatoshi Tanaka, “The Neuroscience of Stress” (Kodansha)
Robert M. Sapolsky, “Why Zebras Don’t Get Ulcers” (Japanese ed.)
American Psychiatric Association, DSM-5-TR (Igaku-Shoin, Japanese ed.)
Stephen W. Porges, “The Pocket Guide to the Polyvagal Theory” (Shunjusha, Japanese ed.)
Haruo Sugi, “What is Stress?” (Kodansha)
Donna Jackson Nakazawa, “Childhood Disrupted” (PanRolling, Japanese ed.)
Nadine Burke Harris, “The Deepest Well” (PanRolling, Japanese ed.)
Masashi Kawano, “Trauma-Informed Care” (Seishin-Kango Publishing)
Yuko Nosaka, “Trauma-Informed Care: Reframing ‘Problem Behavior’” (Nihon Hyoronsha)
Journal Psychotherapy, Vol. 45, No. 3: “Clinical Practice of Complex PTSD” (Kongo Shuppan)
etc.